Nothing in biology makes sense except in the light of evolution--Theodosius Dobzhansky
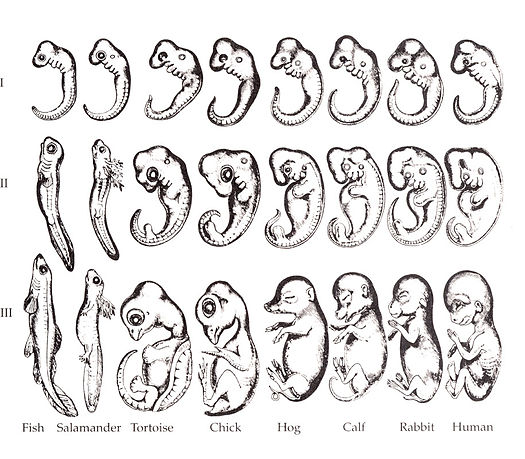
The human embryo is beginning to take shape. It might seem odd that we look a bit wormy at this early stage, and next we will morph into something fishy in appearance. The phrase ontogeny recapitulates phylogeny is hallowed amongst developmental biologists. It means, more or less, our early embryonic stages look like our evolutionary lineage. That is what the famous drawing shown to the left shows: trace our evolutionary lineage (over millions of years), it looks like our embryonic lineage (the 9 months before birth). In this chapter, the human embryo grows gills arches, and re-shapes those gill arches into things more useful to life on land: a mandible and maxilla, ears, and salivary glands (now that we don't have easy access to saline to lubricate every bite of food). Why do we begin resembling worms, then fish, then only much later, little people? Why do we grow gill arches only to replace them? The better question, from the perspective of an evolutionary biologist, is why would we stop developing the way our ancestors did? Would that somehow help us avoid predation, have mor sec, and have superior offspring? A bat's wing, a whale's flipper, a horse's leg and your arm have the same basic pattern (1 bone, 2 bones, 5 bones), even if their size, shape and purpose are different-- you don't need an enrirely new design to turn a leg into a flipper. That's also why the stylish new restaraunt has a new spin on a type of food you already know (asian-fusion!) rather than inventing an entirely new type of food (soylent green!). That's why cars and trucks have 4 wheels, motorcycles have 2, and anything with 3 wheels is nothing more than a footnote in the history of motorized vehicles. Keep in mind we did not evolve from modern-day worms or fish, but the most recent relative a trout and I share resembles the fish more than me, and the most recent relative a trout and worm share resembles the worm more than the trout. Now reverse that: our embyronic stages initially look wormy, then fishy, then lizardy, and finally mammally. The fact we haven't ditched these parasitic stages must mean there is no evolutionary benefit to not look like a fish when we develop, therefore we keep doing it (yes, I called your kids parasites. Maybe that made you miss the fact i made a teleological argument).
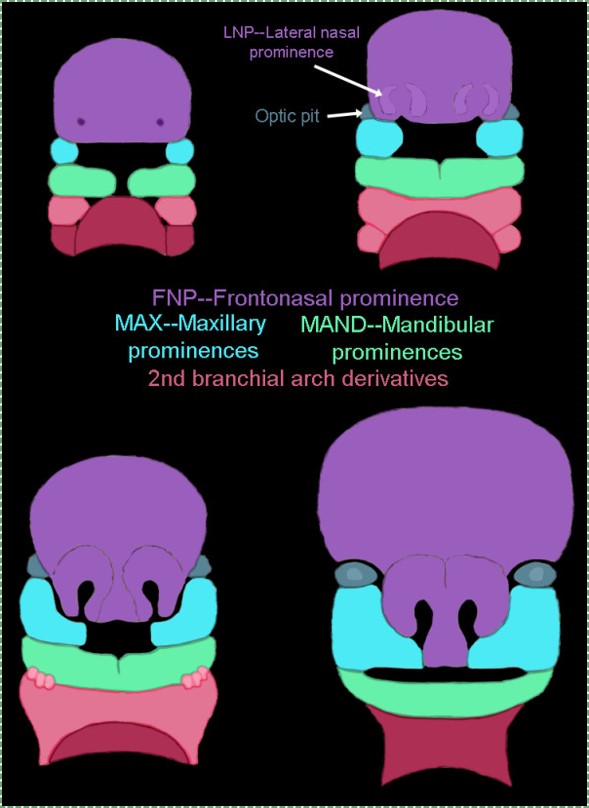
Illustration of the seven facial prominences that give rise to specific regions of the face, by Kristina Aldridge, is liscensed CC BY 4.0
The take-home lesson of the previous paragraph is that human embryos first form gill arches, but quickly remodel them. At 4 weeks, the face begins to develop. It is composed of several parts (or prominences), listed below. Initally, the head develops branchial arches (or pharyngeal archeswhich is technically moe accurate for non-fish), which are paired segmental bulges surrounding the primitive pharynx. These paired bulges will grow across the face and fuse with their partner. One pair of pharyngeal arches will try to fuse, but run into into a big bump called the fronto-nasal process, and fuse with it instead. If we were fish, the arches would become gills instead. In humans, the branchial arches are fated to become a number of cool things, including the teeth.
Mandibular (1st) arch
Maxillary process
Fronto-nasal process
Hyoid (2nd) arch
Development of the face (external)
Formation of the branchial arches
At the 4th week, the primitive gut has not yet fused with ectoderm, so no oral or nasal cavities exist yet. Where the mouth will form is visible, an invagination of ectoderm known as the stomodeum (primitive mouth) is forming. A thin membrane, the oro-pharyngeal membrane (or bucco-pharyngeal), seperates the stomodeum from the primitive pharynx. The primitive pharynx is lined by endoderm. Localized release of morphogensinduces growth of the 3 germ layers, which differentiate into a series of branchial arches. Between each of these new bumps on the outside of the embryo are pharyngeal grooves. On the inside of the primitive pharynx, opposite of the pharyngeal arches, localized growth forms invaginations known as the pharyngeal pouches. These structures appear one pair at a time, from anterior to posterior, and their fate is listed below:
Arch #
Name
Ectoderm and neuro-ectoderm fate
(associated groove)
Mesoderm and neuro-mesenchyme fate
Endoderm (pouch) fate
1st
Mandibular arch
Maxillary process --> upper lip epidermis
n/a
Dermis, maxilla, zygomatic, palatine, vomer
n/a
Lower lip epidermis, Trigeminal nerve.
External acoustic meatus
Dermis, mandible, malleus, incus
Eustachian tube
2nd
Hyoid arch
Epidermis, Facial nerve
disappears
Dermis, most of the hyoid bone, stapes
Palatine tonsils
3rd
Epidermis, Glossopharyngeal nerve
Dermis, the rest of the hyoid bone
Thymus, Parathyroid glands
4th
Epidermis, Vagus nerve
Dermis, Thyroid cartilage, epiglottis
Parathyroid, Thyroid glands
5th
disappears
6th
Epidermis, Vagus nerve
disappears
Dermis, the other laryngeal cartilages
The 1st branchial arch
Next, neural crest cells migrate from the head into the arches and differentiate into special mesenchymal stem cells called neuro-mesenchyme. The neuro-mesenchymal cells release different morphogens which induce localized growth within the mandibular arch, forming the maxillary process. The rest of the mandibular arch grows medially, as does the maxillary process, to form the upper and lower jaw. They grow above and below the stomodeum, which at this time is still not open to the primitive pharynx.
Tissue also grows on either side of the nasal placodes. Two growths in the middle, the medial nasal processes, fuse to form the inter-maxillary segment (or globular process). The growths on the sides form lateral nasal processes, which become the alae of the nose.
Fusion of the 1st branchial arch
The pair of bumps called the mandibular arch form in the 4th week of development and grow medially. They fuse by the end of the 4th week of development, creating a single structure that will become the mandible. For the two halves of the mandibular arch to grow medially, mesenchyme must be removed. This requires induction of the gene for the enzyme hyaluronase, which digests Hyaluronic Acid found in ground substance. This allows epithelial cells to fuse with epithelial cells from the other half of the arch. Fusion requires matching cell-adhesion molecules and desmosomes. The mesoderm of one arch will also fuse with mesoderm of its partner, which requires matching the correct integrin to fibronectin. Later, the mandible will form from 4 seperate parts. The left and right ramuses grow by endochondral ossification from cartilage that is derived from th neuro-mesenchyme that induced the arch to develop in the first place. The body develops by intra-membranous ossification from a left and right pair of ossification centers fromed from the dense connective tissue derived from mesoderm. This will create a cartilage-containing synovial joint between the ramus and temporal bones (the tempero-mandibular joint), and a fibrous joint between the two halves of the mandible which will fully ossify.
Fusion of the maxillary process
The pair of maxillary processes grow medially in the 4th week, but run into the inter-maxillary segment and fuse with it by the 10th week of development. The upper lip, therefore, is formed of three parts (the left and right maxillary proceseses, and the inter-maxillary segment) while the lower lip just two (the left and right mandibular arches). The philtrum is the middle section derived from the medial nasal process. It does not serve a function in humans, it just happens to be there (kind of like my choice of wood in the record player shelf I built) because of how we developed. Many anatomy textbooks have a deep love of describing the functions of organs based on their adult form. I've read some that have tried to describe the function of the philtrum based on its shape and location. They should learn to love development (ontogeny) and evolution (phylogeny), anatomy makes more sense that way.
Fate of the pharyngeal grooves and pharyngeal pouches
If you were a fish, the pharyngeal grooves would have developed into your gills. But as creatures of the land, these structures are either removed or develop into more useful things. Between the mandibular and hyoid arches, the 1st pharyngeal groove invaginates further and forms a tube that becomes the external acoustic meatus. It is lined by ectoderm. The other pharyngeal grooves disappear. One the other side, within the primitive pharynx, the pharyngeal pouches invaginate and grow towards the grooves. The 1st phayngeal pouch elongates into a tube that is fated to become the Eustachian tube, connecting the pharynx to the middle ear (the internal acoustic meatus forms after bone tissue grows around cranial nerve VIII, connecting the inner ear to the brain). The Eustachian tube is lined by endoderm. The mesoderm and neuro-mesenchyme between these two tubes forms middle ear structures, including the malleus, incus and stapes bones.
The other pharyngeal pouches invaginate and form tonsillar and glandular tissue. If you remember GAP, this mnemonic may help you to remember the names of these structures from external to internal: Groove, Arch, Pouch. Or, if you prefer the name pharyngeal cleft rather than groove, the mnemonic becomes CAP.
Development of the palate and other internal structures
Formation of the pituitary and mouth
Inside the stomodeum, a single invagination of ectoderm forms, along the medial portion of the roof (so far, all of the processes and pouches have been left/right pairs). This invagination is named Rathke's pouch. It grows and meets a downward budding of neuro-ectoderm. These two fuse to form the pituitary gland. The ectoderm forms the glandular half (adenohypophysis), and the neuro-ectoderm forming the infundibulum and neural half (neurohypophysis) of the pituitary gland. Rathke's pouch fills in as the two halves of the pituitary fuse, but it is possible a small depression will remain.
Shortly after the lips begin forming, the palate begins to form as well, which begins to divide the newly-formed primitive oro-nasal cavity. The palate has 3 parts that fuse with each other, and with the nasal septum. The primary palate grows from the inter-maxillary segment, and two palatal shelves grow from the maxillary process.
Structure
Lineage
Forms during:
Fuses with
Primary palate (pre-maxillary segment)
inter-maxillary segment (globular process)
6th week
Secondary palate: 9th week
Secondary palate (Palatal shelves)
Maxillary process
7th week
The other palatal shelf: 9th week
Primary palate: 9th week
Nasal septum: 12th week
The first part of the palate to form is the primary palate, which develops from the inter-maxillary segment. When it forms intially, it partially divides the future oral and nasal cavities. Next, two palatal shelves grow off of the maxillary processes. The palatal shelves first grow inferiorly, then change direction and grow medially. At this time, the developing tongue must move out of the way. This allows the palatal shelves to meet and fuse with the primary palate, as well as each other. The fusion happens in an anterior-to-posterior direction. All of this growth is directed by morphogens, such as Fibroblast Growth Factors (FGFs), Bone Morphogenetic Proteins (BMPs), and Sonic Hedgehogs (SHHs).
Maxillary incisors develop from the primary palate, while the canines, pre-molars and molars develop from the secondary palate. At the site where the primary palate and the two palatal shelves fuse, a small hole remains, named the incisive foramen. The oral mucosa above this foramen has a bump named the incisive papilla. Where the two palatal shalves fuse leaves a ridge named the median palatine suture. This creates a visible ridge on the overlying oral mucosa called the (median) palatine raphe.
Keep in mind that we are referring to the entire palate. Much later, anterior portions of the palate mesoderm undergo endochondral ossification and form the palatine bones and the palatine processes of the maxilla (the hard palate). The rest of palatal mesoderm differentiates into muscle tissue, forming the soft palate. Time out for spelling: this is the palate, not an artist's palette of colors, nor a pallet used in shipping, not even a plate on which we place a tasty dinner. Therefore, foodstuffs shipped on a pallet, cooked by a chef with a harmonious pallete, served to us on a plate, will be enjoyed for their flavor when they hit our palate because we have a refined palate (an appreciation for flavor). Got it? English is fun.
The nasal septum is growing inferiorly at this time. It fuses with the completed palate around the 12th week of development. This creates paired nasal cavities.
Development of the tongue
Tongue development begins during the 4th week, just after the branchial arches fuse. Tongue mucosa develops from the endoderm and neuro-mesenchyme of the first 4 branchial arches (skipping the 2nd), while the muscles of the tongue develop from somitic mesoderm. Formation of the tongue involves proliferation of these tissues, followed by fusion of the branchial arches, followed by apoptosis of some tissue to give the tongue mobility.
At the 4th week, the branchial arches fuse along the floor of the future oral cavity. Two lateral lingual swellings proliferate off the 1st arch, followed by a single triangular-shaped tuberculum impar. As these swellings grow, the 3rd and 4th arch develop a swelling named the copula, which grows over the 2nd arch. The oral mucosa of the anterior 2/3 of the tongue is derived from the endoderm of the 1st branchial arch, the posterior 1/3 from the 3rd branchial arch, and the base of the tongue from the 4th branchial arch. Fusion of these structures occurs during the 8th week. The median lingual sulcus forms, where the paired lingual swellings fuse, and the sulcus terminalis forms where the 1st and 3rd branchial arch fuse.
Apoptosis of tongue tissue on the ventral side leaves the tongue attached at the base, and more free to move around. Apoptosis does not remove all the tissue on the anterior portion, a small amount of mucous membrane will remain named the lingual frenulum. An invagination forms posterior to the sulcus terminalis and grows deeper, forming the thyroid gland. This process is similar to the way the anterior pituitary forms. It leaves behind a small depression named foramen cecum, which is a confusing name becuase foramen means hole, but this foramen fills in most of the way, making it more of a pouch. Like Rathke's pouch, it serves no purpose in humans, it's a remnant of the way epithelial tissue proliferates.
Clinical applications of pharyngeal arch development
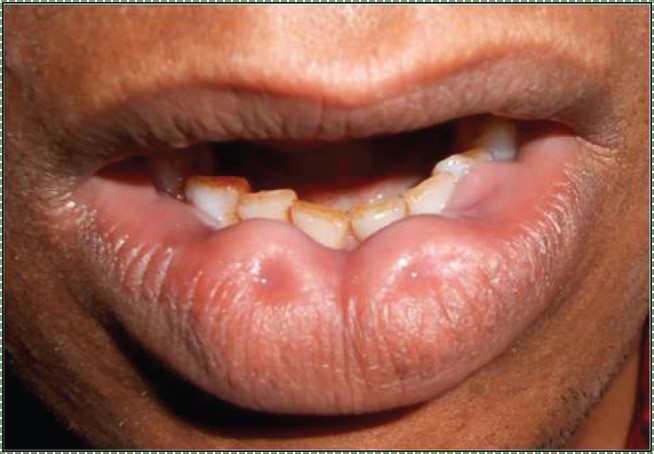
Incomplete fusion of the branchial arches leads to a number of conditions, some more severe than others. Two benign condictions include a lower labial pit, which forms when the two mandibular arches fail to fuse completely. Comissural lip pits may form between the maxillary processes and mandibular arches. These are examples of cosmetic variations rather than congenital malformations.
own work by James Heilman, MD is liscensed CC BY-SA 4.0
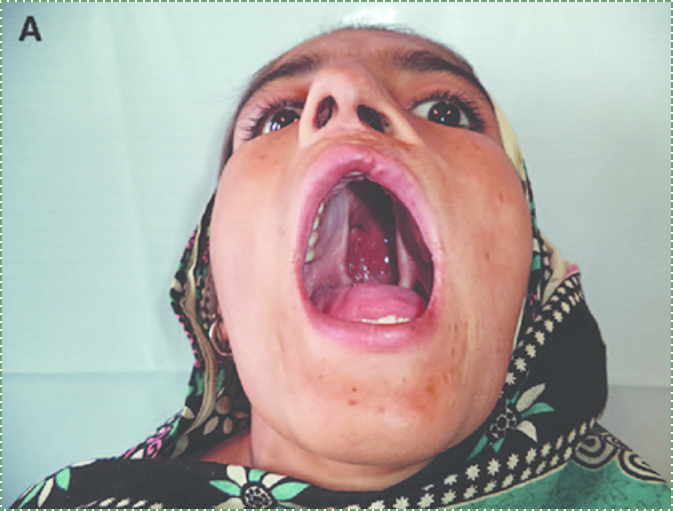
Cleft lip
Incomplete fusion of either maxillary process with the inter-maxillary segment leads to the formation of a cleft lip. This can occur either on the left, right (unilateral) or both (bilateral) borders of the philtrum, although a left unilateral cleft lip is the most common. Cleft lips are more common and more severe in male children. A cleft lip may be accompanied by a cleft palate.
Cleft lip and palate occur in about 1 in 1000 births, making them a relatively common congenital malformation. Risk factors include older mothers, mothers who smoke during pregnancy or take certain medications (e.g. some anti-convulsants). There are many genetic risk factors for cleft lip and palate, some examples are listed below:
Allows epithelial cells to connect during fusion of the lip or palate
A cleft lip can cause difficulty with nursing, as it hinders the formation of a good seal around a nipple. With proper instruction, babies with cleft lip can be breast-fed or bottle-fed using a regular bottle. A cleft lip may cause problems with learning speech. Learning how to speak requires mimicking sounds, because a cleft lip alters vocal sounds, it interferes with sucessful mimicry. Speech and hearing therapy help alleviate these problems. An increased risk of oro-nasal infections is also a concern. The preferred treatment for cleft lip is to seal the gap with surgery at 10 weeks of age. Surgery can leave behind a scar, but otherwise is highly sucessful.
Incomplete fusion of the primary palate and/or the palatal shelves leads to a cleft palate. A cleft palate may or may not be accompanied by a cleft lip. Cleft palate is more common in females.
Cleft palate causes difficulty with nursing, because a child cannot create suction with an opening from the oral cavity into the nasal cavity. There are a number of specialty bottles that help babies with cleft palate bottle feed. Similar to cleft lip, a cleft palate can lead to difficulty learning speech. Disruption of palate formation may lead to shape changes in the Eustachian tube, which in turn alters the abilitty to regulate middle ear pressure and leads to an increased risk of hearing loss.
The preferred treatments for cleft palate include Naso-Alveolar Molding (NAM), followed by several surgeries. NAM involves screwing an appliance at around 10 months of age into the maxilla to slowly pull it forward. Using such an appliance can reduce the amount of surgery to correct the cleft, and instead rely more on the guided growth of a child. The device will need to be adjusted by an orthodontist every two weeks for about a year. Multiple surgeries are required for the treament of cleft palate-- it is complicated region, made all the more complex by the fact is is growing fast at this age. Unfortunately, it is not ideal to wait for a child to stop growing, as a child cannot learn to speak as well later in life.
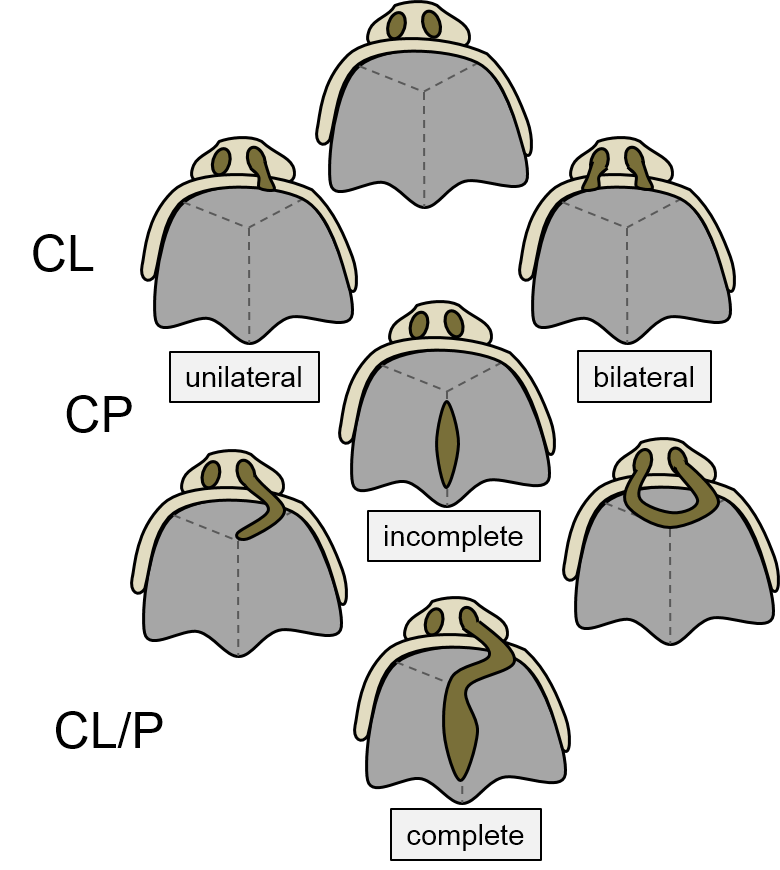
Cleft lip and/or palate are categorized first as being a cleft lip (CL), a cleft palate (CP), or a cleft lip and palate (Cl/P). A unilateral cleft lip or palate affects just the left or right side, while a bilateral cleft affects both sides. An incomplete cleft palate involves incomplete fusion between the primary palate and a palatal shelf, while a complete cleft alsso involves incomplete fusion between the two palatal shelves.
A cleft uvula is the least complicated form of cleft palate, and should be considered a cosmetic variation rather than a congenital malformation.
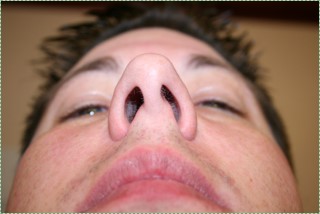
Nostrils before by Jeff and Mandy G is liscensed CC BY SA 2.0
Deviated nasal septum
If the nasal septum grows at an angle as it is developing, it leads to a deviated septum (In fact, it is rare for the septum to develop in a perfectly symmetrical fashion. 80% of people have some nasal deptum deviation, usually without symptoms). The paired nasal cavities contain erectile tissue below the mucosa, which undergoes a nasal cycle, alternating between one side swelling shut and the other remaining open for breathing. This prevents the nasal cavities from drying out from constant use. But for someone with a significant nasal septum deviation, it leads to difficulty breathing when the larger cavity swells shut. A reltively simple surgery called septoplasty can be done to increase the size of the smaller nasal cavity. Septoplasty is not the same as the plastic surgery procedure rhinoplasty, where the shape of the nose is altered.
Excessive growth of the palatal shelves can create a palatal torus, another example of a cosmetic variation. A palatal tosur has no treeatment, as it does not cause any health-related issues. A mandibular torus, however, can develop later in life, often as a response of bone tissue to bruxism.
Ankyloglossia is the persistence of tissue anchoring the tongue to the floor of the mouth. Most of the ventral side of the 1stbranchial arch should undergo apoptosis, leaving behind a small lingual frenulum. However, with inadequate apoptosis, a pronounces lingual frenulum results, limiting the mobility of the tongue. This will cause problems with learning speech, but it is easily correctible with a minor surgery.
Branchial cleft cysts form when incomplete fusion of neighboring branchial arches leaves a remnant of a pharyngeal groove. These usually form a painless mass in the neck, until an infection occurs. No treatment may be done, or they can be removed by surgery. This involves removing the extranous ectodermal (epithelial) tissue trapped deeper in the neck. Whether surgery is or isn't performed may depend on how close the cyyst is to the carotid artery, internal jugular vein or facial nerve.
Rathke's cleft cyst
Similar to branchial cleft cysts, a cyst may form from incomplete oblivteration of Rathke's pounch during formation of the pituitary gland. This leads to a mucus-filled cyst near the anterior pituitary. Due to its location, it can put presure on the optic chiasm, leading to visual disturbances, otherwise it will be asymptomatic. Drainage is the preferred treatment over removal, owing to how close it is to the pituitary gland.